What to Measure In Measurement-Based Care
Description
Now that we have agreed (hopefully) that Measurement-Based Care (MBC) is a method that improves psychotherapy outcomes, we are faced with the logical next question: What should be measured?
Over the years, specific instruments have been developed and used for MBC, including the Outcome Questionnaire (OQ), Treatment Outcome Package (TOP), and the Outcome Rating Scale (ORS), among many others. Some commonly used measures for MBC involve assessing symptom level (for example, the Symptom Checklist, SCL-90 or abbreviated measures). Other MBC measures assess various aspects of the process of psychotherapy, particularly the therapeutic alliance. All of the instruments have some advantages and disadvantages.
At CarePaths, we selected measures and procedures according to several principles:
- The measures must be reliable and valid.
- The measures must be short and easy for patients to complete.
- The measures must be comprehensive, measuring important aspects of mental health and the therapy process
Here’s what we settled on:
Symptoms:
The most prevalent mental health disorders are depression and anxiety. Most mental health disorders are characterized by elevated levels of depression and anxiety. It is essential therefore to assess symptoms of anxiety and depression. We have chosen the two most widely used and accepted measures:
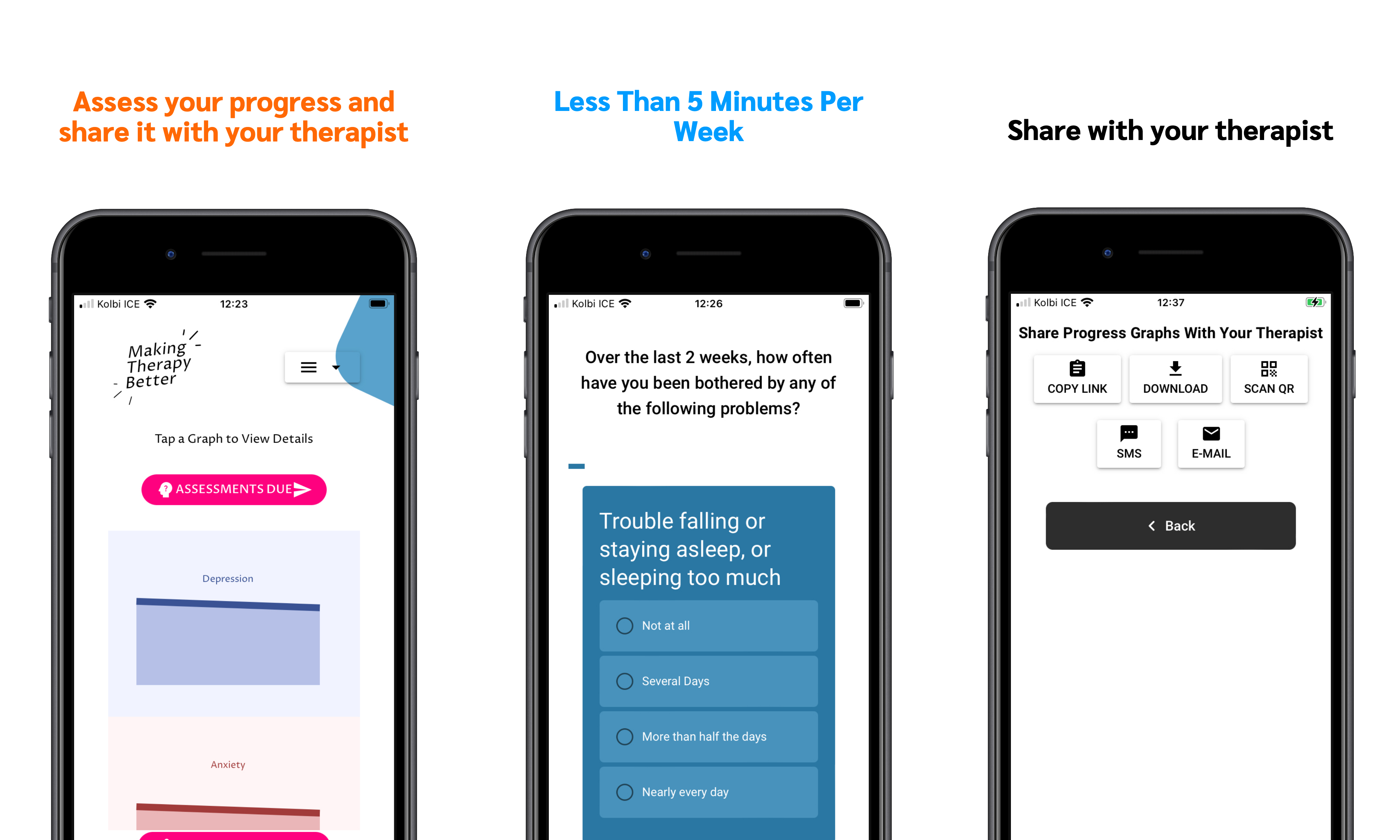
- Public Health Questionnaire-9 (PHQ-9): The PHQ-9 contains nine items assessing symptoms of depression. For each preceding week, the patient rates whether symptoms occurred not at all, several days, more than half of all days, or nearly every day.
- General Anxiety Disorder-7 (GAD-7) The GAD-7 measures symptoms of anxiety. For each preceding week, the patient rates whether symptoms occurred not at all, several days more than half of all days, or nearly every day.
Well-being and Loneliness
Most patients come to therapy seeking much more than a decreased symptomatology. Generally, patients desire greater well-being and decreased loneliness. It is established that perceived loneliness increases risk for mental as well as physical illness and places individuals at as much or more risk for death than smoking, obesity, lack of exercise, and excessive drinking. This has led us to include the following two instruments:
- World Health Organization Well Being -5 (WHO-5). The five items assess general well-being (cheerfulness, calmness, vigor, restfulness, and interest in daily activities).
- UCLA-3 (modified) Loneliness. The three items, plus one we added, assess the patient’s perceived loneliness (lack of companionship, feeling left out or isolated from others, and feelings of loneliness).
Alliance, relationship, and perceived belief in treatment
There is strong evidence that humans have evolved to make judgments of others along two dimensions: warmth and competence. These two dimensions are critical in medicine and psychotherapy. Basically, does the patient perceive the clinician (a) to be trustworthy, caring, genuine, and willing to work in the patient’s best interest, and (b) is the therapist competent to perform the treatment, meaning that the patient perceives that the treatment, as administered by the clinician, will be effective. We use two scales here:
- Confidence in the therapists (3 items):
- My therapist explains my problems in a way I understand.
- I feel accepted and respected by my therapist.
- My therapist is dedicated to helping me overcome my difficulties.
- Confidence in the treatment (3 Items)
- Overall, I expect much improvement as a result of treatment.
- If I do what’s expected of me in therapy, I have a good chance to deal with my problems.
- I think what we do in treatment will help me achieve the changes I want.
Conclusion
These three sets of measures, albeit brief, provide critical information that will be helpful to the therapist and to the patient to assess the process and outcome of therapy. Integrated into therapy and combined with the clinical judgment of the therapist, this information will be useful for understanding progress, modifying treatment, strengthening the relationship, and planning termination and referral.
In my next two entries, I will discuss some of the procedural details of this particular MBC protocol, as well as exercising clinical judgment in interpreting and acting on the data collected.
Join Us Feb. 17 for a Live Interview & Q&A with Bruce Wampold PhD & Scott Miller PhD
Similar posts
-
New App Shows What's Working in Psychotherapy
Bruce Wampold, PhD -

How to Talk to Your Therapist About Your Progress in Therapy
Bruce Wampold, PhD -
Why Using this App can Make Your Therapy Better
Bruce Wampold, PhD -

Using Measurement-based Care (MBC) to Make Clinical Decisions
Bruce Wampold, PhD -

Talking to Patients as Part of Measurement-Based Care
Bruce Wampold, PhD -

Dr. Bruce Wampold on How to Make Therapy Better
Bruce Wampold, PhD -

Administering Assessments: The Pragmatics of Measurement-Based Care (MBC)
Bruce Wampold, PhD -
An Introduction to CarePaths’ Approach to MBC
Bruce Wampold, PhD