Dr. Bruce Wampold on How to Make Therapy Better

Description
This interview was conducted at the Request of Jordan Harris, Ph.D, LMFT, LPC who offers his own counseling services as well as resources for other counselors at www.jordanthecounselor.com.
In his words:
“Bruce Wampold is the Rocky of the therapy world.
Coming from the world of math and science, you could say he was an unlikely candidate to become a major player in the touchy feely world of therapy.
But that didn’t stop him from bringing a hard science approach to psychotherapy and becoming one of the most important voices in the field.
And now, like Rocky mentoring Creed, Wampold is paving the way for the next generation through Making Therapy Better.”
First question: Briefly, how did you get into the field of psychology from where you started in mathematics?
As an undergraduate, I was a mathematics major and mathematical economics minor.
I loved the sciences, and I loved the beauty and rigor of mathematics. I was still quite naive about the field of psychology. When I graduated in the early seventies, I didn’t know what I wanted to do, so I decided to teach for a few years while I figured it out. I became a junior high school math and science teacher and later a math teacher and wrestling coach at Punahou School in Honolulu.
Punahou was a fascinating yet challenging environment– very multicultural. I became interested in how some students achieved despite significant challenges, and others failed to thrive even though they had great privilege.
And so I enrolled in a master’s degree at the University of Hawaii in school counseling, which only increased my interest in psychology, especially the fact that so much of our understanding of the world comes from psychology. Realizing that this was the field I was really drawn to, I went to the University of California at Santa Barbara for the Ph.D. program in counseling psychology.
What attracted you to the research side of things?
Well, that’s interesting.
When I started graduate school, I wasn’t planning to continue in research. I wanted to practice as a psychologist to understand people and their challenges. Of course, I had to take research and statistics courses, which appealed to my interest in mathematics. More importantly, I came to understand how important the research is for understanding how psychotherapy works and how it can be improved.
Reading the research from that time, I came across so many conclusions that I felt weren’t justified scientifically. Perhaps a little immodestly, I thought I could do a better job than most of the people who were doing research at the time.
But more than that I really wanted to contribute to the field, and research was a way to make a contribution that went well beyond seeing patients one at a time.
Some of your major contributions to the field have been the contextual model of psychotherapy and the common factors understanding of what makes effective therapy. Can you briefly describe these ideas, how you discovered them and why they’re so important?
That’s a great question.
It was somewhat by happenstance that I got interested in the common factors and the development of the contextual model.
I was teaching a course when I first came to the University of Wisconsin in 1991, using the Handbook of Psychotherapy and Behavior Change as the course text. Several chapters maintained that there were certain treatments that were more effective than others. In particular it taught that cognitive behavioral therapy was a superior treatment for many disorders, such as anxiety and depression.
I didn’t want my students to take for granted that the authors had synthesized the research in an appropriate manner. So, what I did was assign students to read a particular chapter as well as the original research on which the chapter was based.
Over and over again, the students reported back that while the chapter contends that cognitive behavioral treatments are superior to other treatments, the research doesn’t seem to justify that conclusion.
That was disturbing to me for two reasons.
First of all, it offended me as a scientist. I knew from my training that we should be faithful to the evidence and not let other factors, such as our own advocacy of a particular treatment or some kind of political or professional affiliation, determine the conclusions.
The other part was more personal, in that I had benefited from psychotherapy in my life, and it wasn’t cognitive behavioral therapy. It offended me that the conclusions were saying that one particular treatment was more effective than another when that was not the case– or least was not shown persuasively by the evidence.
My research group and I realized that it was time to do a meta-analysis of all the studies comparing two or more legitimate treatments, to look at the question of relative efficacy in the most rigorous way possible.
Making several innovations in the meta analytic approach, we undertook this immense and comprehensive review of the studies that compared two or more treatments and the results were absolutely clear.
We found no evidence that any one treatment was superior to another.
We published the study in 1997 and there was some strong reaction to it, but there was also much support for it.
People said, “This is great because this is what we suspected and somebody finally analyzed the data with absolute rigor and came to the same conclusion.” We weren’t the first to reach that conclusion, but we established it more comprehensively and rigorously than had been done before.
Soon thereafter, I was approached about writing a book for Lawrence Erlbaum Publishers based on that meta analysis and the extant research.
In the course of doing research for that book, it became clear that we needed a model of how the various psychotherapies work based not only on the science of psychotherapy, but incorporating evidence from placebo studies, cultural psychiatry, anthropology, social psychology and so on. I developed with my students, prominently Zac Imel, a contextual model of psychotherapy.
The Contextual Model stipulates that three pathways contribute to the effects of psychotherapy. The first pathway involves the caring, attentive, real and empathic relationship.
The second pathway involves the belief that the hard work of therapy will lead to distress reduction and increased well-being; that is, confidence in the treatment leads to expectations of change.
The third pathway involves the specific ingredients of the treatment.
All treatments persuade the patient to participate in life in a more adaptive manner. Over the years many of the conjectures that emanate from the contextual model have been supported by further research.
When did you become interested in deliberate practice and measurement-based care?
I had come to the conclusion that training in particular treatments to the exclusion of relationship and common factors included in the contextual model was not the proper way to improve the quality of mental health services. And of course that’s my ultimate goal, to use the research to actually improve services.
So, I wrote a paper with one of my students that attempted to answer the question: if we give up the belief that some treatments are superior to others, what is the alternative for improving outcomes?
At that time, the only viable alternative was the idea of providing the therapist with feedback about patient progress, so they can adjust therapy appropriately to achieve better outcomes.
Mike Lambert and Scott Miller, among others, had done much research showing that providing feedback will improve the quality of services. After reading the research I became convinced that measurement-based care needs to be used in all mental health services.
At the time, I wasn’t involved in measurement-based care, but I recognized it as an important way to improve the quality of mental health services. And since then, Jamie Delgadillo in England, Kim De Jong in the Netherlands, and others have produced convincing research that measurement-based care is a viable way to proceed.
Now, there are a couple of caveats to this idea.
One is that it’s really important how measurement-based care is implemented. There are instances in which the implementation is not carefully done and the quality of the services really doesn’t improve. So the manner in which measurement-based care is implemented is absolutely critical.
The other part is that even in the best of circumstances, it appears that therapists who get feedback about their patients’ progress don’t actually improve their skill. That is, therapists, even when they receive this information, don’t improve over time. This led me to think about what we could do to provide therapists the opportunity to actually improve.
I’d been reading about deliberate practice, and I found it intriguing.
As you know, there are experts in many fields, such as athletics, music performance, surgery, and so forth. Anders Ericsson, a professor at Florida State University, who recently passed away, studied what makes an expert.
His astounding research demonstrated that what characterizes experts, who may or may not have natural talent, is deliberate practice. Experts deliberately practice the skills that are necessary for expert performance, and continually improve.
We didn’t have anything like deliberate practice in psychotherapy, so it is not surprising that therapists were generally not improving.
Professor Ericsson’s work has led a number of us, including Scott Miller, Darryl Chow, Tony Rousmaniere, and myself, to identify the skills that make effective therapists so they can practice them deliberately in the way that Erickson talks about.
Deliberate practice involves identifying the skill to be practiced (say empathy with challenging patients), setting goals for performance of the skill, and iterative practice with feedback from an instructor, supervisor, or coach.
So measurement-based care, if implemented well, tends to have an overall improving effect on client outcomes, but even with MBC an individual therapist may not improve over time without deliberate practice?
Yes, absolutely. The critical first step is to gather information about how we’re doing as therapists.
You can’t improve at any skill if you don’t know how successful you actually are. And therapists really can’t make that determination without having some information.
But information alone isn’t sufficient to improve as a therapist. You have to take that information and use it to improve your therapeutic skills.
So the next step, and it’s a difficult next step, but an important one, is to ask, what skills do I need to practice to continue improving my outcomes with patients?
How does your current work with CarePaths continue some of the major themes of your career?
When CarePaths approached me about this project, Making Therapy Better, I was intrigued because this is what I’ve been thinking about for the last decade or so of my career. What can we implement in practice settings that will improve the quality of service for patients?
I’m retired from my university position, but I still want to be involved in the field doing something important. So the opportunity to collaborate with an organization that works with many therapists was very attractive.
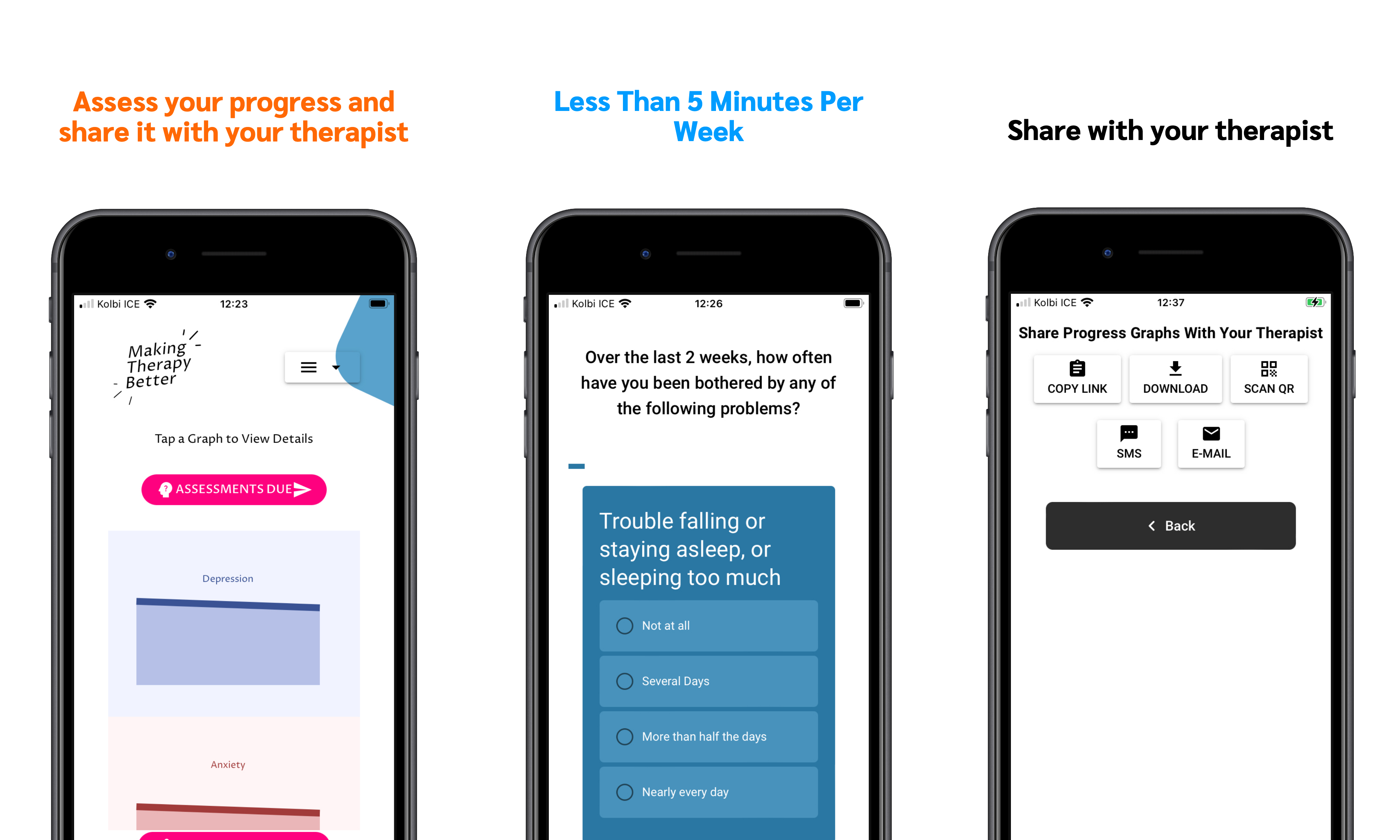
Our first initiative was designing a measurement-based care platform for therapists to use, which I think we’ve done in an innovative way. We’ve made some changes that are improvements over the way other organizations have implemented MBC.
In addition to the tools we are developing, which are part of the CarePaths EHR software, we have created a standalone site for Making Therapy Better, where we’ve already hosted a webinar with free CEUs, several blogs, and an index of academic research on measurement-based care.
We’re about to start a podcast where I discuss different aspects of improving therapy with important figures in the field.
What are some of your hopes for the Making Therapy Better project and for the future of psychotherapy?
We know that psychotherapy is effective.
There’s definitive research showing that psychotherapy is as effective as medications for most mental disorders without the side effects, and it’s more resistant to relapse. However, not every patient benefits from psychotherapy
Consequently, the goal is to find ways to make therapy even more effective, ideally without burdening the therapist or patient.
MBC is the first and most critical step. We need information about how patients are progressing to adjust therapy accordingly.
The next step is using deliberate practice to improve particular therapeutic skills.
Both of these initiatives are to a large extent technology-based. This raises the issue of how mental health services will use technology to improve. In general, I would like to see technology used to its fullest potential to improve the quality of care.
I certainly don’t predict that psychotherapy will become obsolete– technology cannot replace the social healing aspects of psychotherapy. But I do think there are really helpful ways to integrate electronic applications with psychotherapy beyond MBC. For example, there might be an app that lets patients practice different skills that have been assigned by the therapist over the week.
Another area that’s really important is social media and digital communities.
Therapists, particularly in private practice, work in varying degrees of isolation. Technology can provide opportunities for us to work together to improve our skills and outcomes. We’re hoping that Making Therapy Better becomes one such community.
The world is changing, and with each new step, we have the choice to embrace it or catastrophize it as the end society as we know it.
Written language changed the world in ways that many thought was catastrophic.
The adoption of computers and other devices,caused many to lament the end of books and reading.
The idea of social relations involving face-to-tace interactions has been altered dramatically.
Each major transition presents challenges, as well as exciting opportunities. We’ve managed to evolve in response to these challenges as a species and we have to do the same within the field of psychotherapy.
Join Us Feb. 17 for a Live Interview & Q&A with Bruce Wampold PhD & Scott Miller PhD
Similar posts
-
New App Shows What's Working in Psychotherapy
Bruce Wampold, PhD -

How to Talk to Your Therapist About Your Progress in Therapy
Bruce Wampold, PhD -
Why Using this App can Make Your Therapy Better
Bruce Wampold, PhD -

Using Measurement-based Care (MBC) to Make Clinical Decisions
Bruce Wampold, PhD -

Talking to Patients as Part of Measurement-Based Care
Bruce Wampold, PhD -

Administering Assessments: The Pragmatics of Measurement-Based Care (MBC)
Bruce Wampold, PhD -
What to Measure In Measurement-Based Care
Bruce Wampold, PhD -
An Introduction to CarePaths’ Approach to MBC
Bruce Wampold, PhD